Malaysian cardiologists have begun a groundbreaking study into an innovative device designed to treat one of the most challenging problems in modern heart medicine: severely calcified plaque blockages in coronary arteries. The research, spearheaded by consultant cardiologist Datuk Dr Tamil Selvan Muthusamy, represents a significant step forward in addressing a treatment gap that has long frustrated cardiac specialists across Southeast Asia and beyond. The technology, called the Hertz Contact-IVL System, promises to improve outcomes for patients whose plaque has hardened to the point where conventional interventions struggle to succeed.
Coronary artery disease—the buildup of plaque inside blood vessels that supply the heart—remains a leading cause of death and disability worldwide, including across Malaysia and the region. Plaque itself is not a simple substance but rather a complex accumulation of fatty deposits, cholesterol, calcium, cellular debris, and fibrin, a protein involved in blood clotting. Over years and decades, this material deposits on artery walls, progressively narrowing the vessels and restricting blood flow. When plaque buildup becomes severe, it can completely block blood supply to portions of the heart muscle, triggering heart attacks, heart failure, or strokes that can be fatal or cause permanent disability.
For decades, cardiologists have managed coronary artery disease through a three-pronged approach combining lifestyle modifications, pharmaceutical therapy, and when necessary, surgical or catheter-based interventions. Among the most common procedures are percutaneous coronary intervention (PCI), in which a catheter is threaded into blocked arteries, coronary artery bypass grafting (CABG), where surgeons create alternative pathways for blood flow, and balloon angioplasty, which physically widens narrowed vessels. These techniques work reasonably well when plaque remains relatively soft; doctors can insert a balloon, expand it to compress the soft material flat against the artery wall, then deploy a stent to hold the artery open. However, when calcium deposits have hardened the plaque into a near-concrete-like consistency, these standard approaches often fail to deliver adequate results.
Severe calcification of coronary arteries presents multiple technical challenges that complicate treatment and worsen patient outcomes. The hardened calcium resists compression from conventional balloon pressure, making it extremely difficult for physicians to achieve adequate expansion of stents. Even when special techniques such as rotational atherectomy—essentially a high-speed drill—or high-pressure balloon angioplasty are deployed, success rates decline and complications increase. Dr Tamil Selvan explains that traditional approaches designed for softer plaque prove inadequate: conventional balloons crush soft material efficiently to create the necessary hollow space within vessel walls for stent placement, yet fail against calcified lesions that stubbornly resist mechanical force.
Intravascular lithotripsy (IVL) emerged several years ago as a transformative solution to this problem. The technology borrows principles from extracorporeal shock wave lithotripsy, a procedure long used to break kidney stones non-invasively. In coronary applications, doctors position a specialized catheter at the site of calcified blockage and generate ultrasonic pulses that create acoustic waves. These pressure waves are transmitted to the hardened plaque, fracturing the calcium deposits into smaller fragments that can then be compressed and managed. The approach represented a genuine breakthrough in treating previously intractable cases of severely calcified coronary disease. Yet even this innovation carries limitations that have prompted continued refinement.
The original IVL systems, while effective, operate within constraints that can limit their utility in complex cases. The number of ultrasonic pulses available is finite—early systems offered only eight pulses, with newer versions providing twelve—meaning physicians must break all the calcium within that pulse budget or accept incomplete revascularization. The catheter hardware itself is relatively bulky, creating delivery challenges, particularly when arteries are severely narrowed with minimal space for the device to pass through. Additionally, IVL systems come in fixed sizes; a three-millimetre balloon cannot adjust to treat vessel segments that vary from 3.5 millimetres at one point to just 2 millimetres at another, a common anatomical variation that forces physicians to use multiple devices or accept incomplete treatment of long calcified segments.
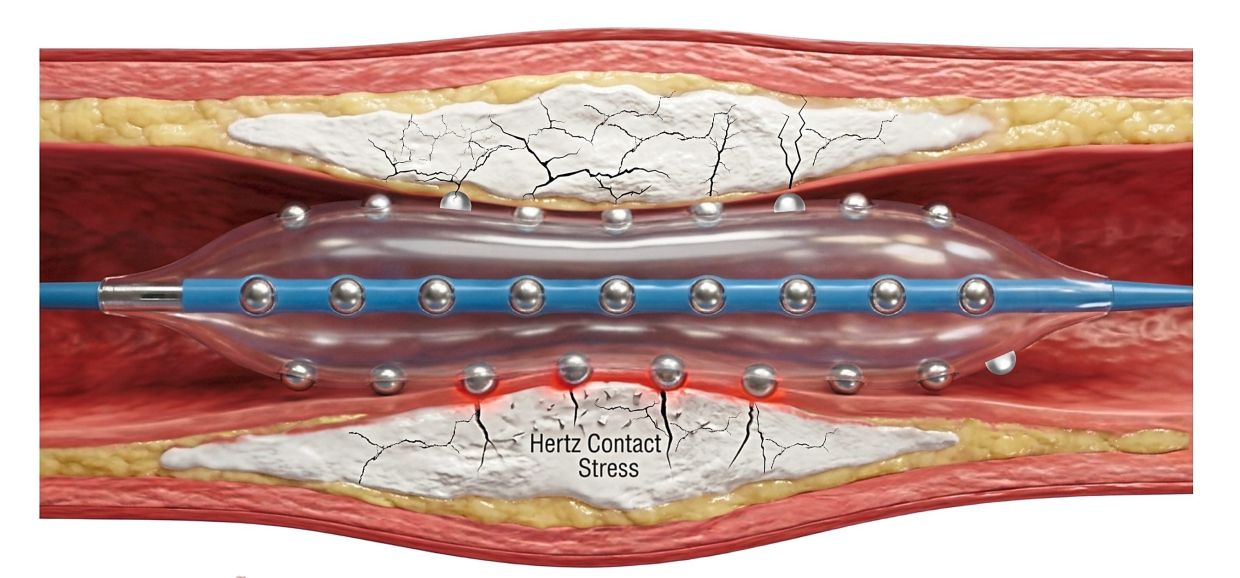
The Hertz Contact-IVL System, which Dr Tamil Selvan's team began studying during 2025, represents an important evolution addressing these limitations. Rather than relying on external energy generators to create acoustic waves, the HC-IVL system employs an elegantly different mechanical approach. The device incorporates a balloon embedded with tiny metallic hemispheres constructed from stainless steel. When this balloon makes contact with calcified plaque and physicians apply pressure, the hemispheres create focal points where pressure amplifies dramatically, transmitting concentrated force that cracks dense calcium deposits without damaging the surrounding healthy tissue. This mechanical transmission of force proves more precise and controlled than acoustic wave energy, allowing deeper, wider cracks in the plaque that facilitate superior stent expansion.
The practical advantages of the mechanical approach extend beyond physics into clinical reality. Because the HC-IVL system does not depend on a fixed number of energy pulses, a single balloon can treat extended calcified lesions or multiple blockage sites, eliminating the need for physicians to swap devices during complex procedures. The catheter's improved deliverability—its ability to navigate through severely narrowed vessel segments—removes a significant barrier that has frustrated treatment of the most challenging cases. The system's adaptability to varying vessel sizes means that physicians need not accept incomplete revascularization due to anatomical constraints. For Malaysian patients with complex coronary disease, particularly those in rural or secondary-care settings where immediate access to tertiary cardiac centres may be limited, such advances could prove transformative.
Dr Tamil Selvan and his colleagues recognized that while the HC-IVL device had undergone preliminary evaluation through small multicenter studies in the United States, the technology required rigorous validation in larger, more diverse patient populations before widespread adoption. Malaysia's sophisticated cardiac infrastructure, combined with the nation's diverse demographic profile and high prevalence of coronary artery disease risk factors, provided an ideal setting for definitive research. The decision to conduct a substantial local study reflects both scientific prudence and regional leadership in cardiac innovation. By carefully evaluating the device's safety profile, efficacy in various patient subgroups, and long-term durability, the Malaysian research team aims to establish evidence that will inform adoption decisions not only domestically but across Southeast Asia.
The implications of this research extend beyond individual patients to the broader economics of healthcare delivery. Coronary artery disease imposes enormous costs on healthcare systems throughout the region, consuming resources for emergency interventions, prolonged hospitalizations, and management of complications from failed initial treatments. More effective first-line therapies that reliably open calcified arteries with fewer complications promise to reduce these downstream costs while improving quality of life for patients. For Malaysia specifically, where coronary disease burden has risen alongside economic development and changing lifestyle patterns, technological advances that enhance treatment success rates address a genuine public health priority.
The Malaysian cardiology community's engagement with cutting-edge device innovation reflects broader trends reshaping cardiac medicine in Southeast Asia. Historically, advanced cardiovascular technologies were developed and refined in Western markets before becoming available in the region, often at considerable delay and cost. By participating in primary device validation studies, Malaysian institutions and researchers position themselves as contributors to global medical knowledge rather than merely consumers of innovations developed elsewhere. This shift toward local leadership in clinical research strengthens the region's capacity for independent evaluation of new therapies and reduces reliance on external validation for adoption decisions. For trainees in Malaysian cardiology programs, involvement in such research provides invaluable exposure to cutting-edge methodology and direct engagement with device manufacturers and international colleagues.
As the Malaysian research team advances its HC-IVL study, several dimensions merit careful attention. The researchers must evaluate not only immediate technical success—whether the device reliably cracks calcium and allows adequate stent deployment—but also clinically meaningful outcomes including symptom improvement, functional capacity restoration, and freedom from repeat revascularization. Long-term follow-up data proving sustained stent patency and durable symptom relief will be essential before the device gains widespread adoption in Malaysian practice. Additionally, cost-effectiveness analysis comparing HC-IVL to existing alternatives remains important, as healthcare budgets in Malaysia and throughout Southeast Asia remain constrained. The study also offers opportunity to identify patient characteristics predicting success or complications, enabling physicians to select appropriate candidates and counsel them realistically about expected outcomes. Through meticulous evaluation and transparent reporting of results, regardless of whether findings prove entirely favorable or reveal unexpected limitations, the Malaysian research team will contribute essential knowledge advancing cardiac care not only domestically but throughout the region.

